Keywords:
Covid-19, makers, innovation
Peter Troxler
Complement: Responses by Dyhrberg Højgaard, Boeva, García and Cuartielles [pdf]
1 Introduction
The worldwide and rapid spread of Covid-19 (officially declared a pandemic on 11 March 2020) led to a number of reactions and effects, such as local and national lockdown measures, increased hospitalisation of patients, and a related surge in demand for different medical and non-medical items which caused interruptions in the globalized supply-chains – and created a hitherto unknown potential for frugal innovation.
The story that served as the opening scene for this development happened in Italy and goes like that: Just two days after the declaration of the pandemic, on Friday, 13 March, in a hospital in Brescia, one particular part of a breathing apparatus (a valve that changes speed and pressure in the airflow, called the “venturi”) broke down and there were no replacement parts available. Through personal connections, the doctors managed to find an engineer at a company specialised in 3D-printed prototypes who was able to reproduce the bestpart within 24 hours. The contact was allegedly brokered by the founder of a fablab and tech supportjournalist, Massimo Temporelli (Corsini et al., 2021; Sher, 2020a). This story made the headlines in the European and global press, and the fablabs and 3D printing were inextricably linked to fixing supply chain tribulations for healthcare.
The people in Brescia extended their work by proposing to use a Decathlon snorkelling mask as an improvised breathing aid at a time when these machines were believed to become a bottleneck in treating Covid-19 patients (Corsini et al., 2021; Sher, 2020b). Makers all across Europe and world-wide started to replicate the piece that would attach Decathlon masks to hospital breathing equipment. That’s how the virus first infected the so-called “maker movement”. Although hooking-up the scuba masks to medical devices proved more difficult than expected, makers globally continued to develop these devices that presumably were short in supply. Other popular items produced by makers included face shields and face masks. As Chalet et al. (2021) note, one particular design of a face shield by Jozef Pruza, a manufacturer of 3D printers well-known and admired amongst makers for their strong open source adherence, strongly contributed to the mobilisation of makers.
Self-organizing groups of makers started to defeat global supply chains by producing supplies locally – particularly personal protective equipment (PPE) – for medical professions and other frontline workers, meeting the ongoing needs of public and private organizations. The realisation that by joining together and self-organising they could manufacture meaningful products for others, rather than just quirky stuff for themselves, quickly became part of the narrative of the self-assumed “maker movement” and the press reporting on it. This was supposed to be the seminal example of how distributed manufacturing could effectively and efficiently rise above the deficiencies of globalized supply-chains and centralized manufacturing and hence contribute to a transition to peer-production of physical goods.
2 Background
2.1. Making as peer-production
In the early 2000s, several prominent figures proposed that a “maker movement” would bring about a tangential development in technology design and production. Neil Gershenfeld (2005) called it “personal fabrication, the coming revolution on your desktop”. The same year, Mark Frauenfelder and Dale Dougherty launched Make: magazine, Massimo Banzi and David Cuartielles presented their first Arduino boards that made microcontrollers easily accessible to artists and tinkerers, and Eric Wilhelm launched the online platform Instructables where people could share instructions on how to make things from as tree houses to 3D printed bionic hands. We called this the “year zero of making” (Boeva & Troxler, 2021, p. 226; Troxler, 2015, p. 61).
This journal has, on various occasions, investigated making as peer-production. We found that shared machine shops were not new, sharing was not happening, or hackerspaces were not open (Troxler & Maxigas, 2014). We studied feminism, making, and hacking (Bardzell et al., 2016) and the institutionalization of shared machines shops within universities and corporations and found that they redefined making’s origins and prospects (Braybrooke & Smith, 2018).
In my own research on making as peer production I have decidedly remained ambivalent. I have been sympathetic to the narrative of making being a form of peer production (Troxler, 2010, 2011). I have acknowledged what fab labs and similar spaces have achieved for technology appropriation, local cultures, and education (e.g. Troxler, 2018). I have highlighted the struggle for polycentric structures and a new peer-production commons in the fab lab community (Troxler, 2013). Adopting a sociotechnical perspective, I have pointed out that there was more needed than the core making technologies – 3D-printing and laser cutting – particularly becoming sustainable, developing the network, embracing a lateral paradigm (Troxler, 2015), eschewing technocracy (Troxler, 2016b), and building a commons (Troxler, 2017, 2019). And I have asked myself what in making as peer-production of open source hardware could become an equivalent to the infrastructure projects known from open source software such as the Apache web server (Troxler, 2016a). So, was peer-producing personal protective equipment for healthcare and related sectors such an infrastructure project?
2.2. Framing the makers’ response as a paradigm change with transition theory
Book titles that invoke a “next revolution” (e.g. Anderson, 2012; Gershenfeld, 2005) allude to something radical happening in their subject area – in this case the manufacturing of things. In science, such revolutions have attracted the interests of philosophers such as Kant and, more recently, Kuhn. In his treatise of “the structure of scientific revolutions”, Kuhn (1962) describes this structure as consisting of four steps – starting with the dominant paradigm active in normal science, emerging anomalies in normal science that lead to extrapolatory activity or “extraordinary research”, the subsequent adoption of a new paradigm that gradually replaces the old one (as its incumbent adepts eventually die), and finally, in the aftermath of the scientific revolution, the new paradigm becoming the new normal.[1]
In the early 2000s, several prominent figures proposed that a “maker movement” would bring about a tangential development in technology design and production. Neil Gershenfeld (2005) called it “personal fabrication, the coming revolution on your desktop”. The same year, Mark Frauenfelder and Dale Dougherty launched Make: magazine, Massimo Banzi and David Cuartielles presented their first Arduino boards that made microcontrollers easily accessible to artists and tinkerers, and Eric Wilhelm launched the online platform Instructables where people could share instructions on how to make things from as tree houses to 3D printed bionic hands. We called this the “year zero of making” (Boeva & Troxler, 2021, p. 226; Troxler, 2015, p. 61)
Similarly, Geels discusses technological transitions as evolutionary reconfiguration processes (Geels, 2002; Geels & Schot, 2007). A central concept in Geels’ model is the sociotechnical regime (p. 1260), as “technological regime” defined by Rip and Kemp (1998):
“A technological regime is the rule-set or grammar embedded in a complex of engineering practices, production process technologies, product characteristics, skills and procedures, ways of handling relevant artefacts and persons, ways of defining problems; all of them embedded in institutions and infrastructures” (p. 338).
Sociotechnical regimes are at the centre of a multi-level perspective on technological transitions. At the meso-level they form a relatively stable patchwork that is embedded in a landscape of slow changing external factors at the macro-level. At the micro-level, novel configurations appear as potentially radical innovation in technological niches.
The central assumption is that societal systems go through long periods of relative stability and optimisation that are followed by relatively short periods of radical change. Transitions come about when the dominant structures in society (regimes) are put under pressure by external changes in society (landscape) as well as endogenous innovation (niche). Such transitions have been found in history, e.g., the replacement of sailing by steam vessels in de second half of the 19th century (Geels, 2002) or the transition in mobility from horse-carriage to automobile (Geels, 2004).
Under certain conditions, seemingly stable societal configurations can transform relatively quickly – i.e., much faster than the 40-60 years in the above examples. Loorbach (2007) for instance gives 15+ years for long-term systemic and cultural change on the macro level, 5-15 years for structural, institutional and regime change at the meso level, and up to 5 years for micro level innovations, e.g., in terms of change of certain practices.
Niche innovations have the potential to change or replace dominant sociotechnical regimes if some preconditions and mechanism come into play.
- A window of opportunity at the regime (meso) or landscape (macro) level, e.g., tensions in the sociotechnical regime, shifts in the landscape
Some mechanisms, according to Geels (2002), are:
- Innovations are gradually stabilising into a dominant design through niche-cumulation, i.e., being “used in subsequent application domains” (p. 1271)
- Technological add-on and hybridisation, i.e., new technologies are used alongside or in combination with old ones to overcome some of their deficiencies or bottlenecks
- Growth in particular (niche) markets where new technologies are preferred over old ones
From an initial analysis, the situation of the Covid-19 pandemic appears to fulfil a number of these characteristics. The pandemic and related supply shortages created a window of opportunity. The technical innovation of 3D printing had found adoption in niches in many sectors – three dimensional visualisations in education, prototyping in engineering design, medical models for planning surgery in healthcare, and amateurs reproducing science fiction figurines. For some applications, 3D printing has become a valid alternative for traditional manufacturing technologies.
The pandemic as a window of opportunities
This window of opportunity for responses to the healthcare crisis has been documented in a wide range of publications. In the context of this study, collections of responses to the supply shortages are particularly interesting. Kunovjanek and Wankmüller (2020) analysed 289 3D printed products made in response to the pandemic which they collected from homepages, company reports, press releases and media articles. 119 of these products were manufactured by some kind of community – both industry-based and volunteer-based, and 195 of product designs were shared.
The Strategic Design Research Journal released a double special issue on “Design contributions for the COVID-19 global emergency”. The first issue collected direct accounts of the hands-on activities of designers, who in many cases worked in one way or another with volunteers, often in 3D printing (Rossi et al., 2020). The second issue collated theoretical and methodological reflections (Rossi et al., 2021). As part of this collection, Moura et al. (2020) collected 113 cases of “design responses” to the pandemic from design blogs, social media and various other sources. Similarly, Galdon et al.(2020) established a design focused collection of “everything” Covid-19 related that appeared in design blogs and specialist websites assembled and categorized over 500 items – maps, charts, visualizations, products, networks, etc. – over the period of the first five months of 2020 and analysed their temporal and geographical distribution (Rodgers et al., 2020).
3D printing as a dominant design in a cumulation of niches
While the spread of “consumer grade” printers has failed to fulfil the early hype prognoses of home printing, 3D printing has certainly become a modern pastime – 25 % of respondents in sculpteo’s “state of 3D printing 2021” indicate their primary context of using 3D printing is personal interest (sculpteo, 2021). Yet, “consumer grade” printers have also found their way into schools and libraries, onto the desks of mechanical and automotive engineers as prototyping tools, into artists’ studios, and into hospitals, where they are used to print anatomical models for planning and explaining surgical interventions or to produce patient specific instrumentation like surgery templates (aka “saw guides”).
Journals like 3D Printing in Medicine, special interest groups of clinicians developing guidelines for medical 3D printing (e.g. Chepelev et al., 2018), 3D print centres at hospitals and hospital trusts, often organised as hub-and-spoke models with 3D research and design labs at for instance a university hospital and printing labs at smaller units, have been around for over half a decade (see e.g. Calvo-Haro et al., 2021).
So, next to the original niche of makers and their shared machine shops, medical and point-of-care 3D printing is another, well-developed niche, that is particularly relevant in the context of the pandemic and produced its own responses to the pandemic (see e.g. Perez-Mañanes et al., 2021; Rybicki, 2021; Tino et al., 2020), often in cooperation with the makers’ niche (see e.g. Frazer et al., 2020; Hartig et al., 2020; Sugrue M et al., 2020; Throckmorton et al., 2021).
3D printing technology as an add-on
In the field of manufacturing, 3D printing has linked up with established technologies of mass manufacturing, particularly casting and injection moulding. 3D printing of sand moulds and cores is common practice in metal casting (see e.g. Thiel et al., 2017). Similarly, tools for injection and blow moulding can successfully made by 3D printing (see e.g. Gunbay et al., 2019).
In some cases, 3D printing even equals mass manufacturing capabilities, i.e., producing several hundred thousand items per day, a throughput that is rather common for injection moulding. For instance, Kunovjanek and Wankmüller (2020) found that 34 of the products were mass manufactured with 3D printing technology.
In the field of healthcare, 3D printing technology also serves as an add-on in a different way. 3D printed models are considered “an appropriate representation or extension of data contained in a medical imaging examination” for certain conditions (Ali et al., 2020; Ballard et al., 2020). Here, 3D printing technology enhances traditional (visual) imaging.
Growth in (niche) markets
A pandemic is by definition a global affair, and its management follows internationally shared patterns – lockdown measures, social distancing rules, ventilation and intensive care of patients – as do the shortages in supply of PPE, spare parts, or oxygen. Likewise, the makers’ response follows a global pattern in a medially globalised world. However, national implementations of global patterns differ nationally and even across administrative regions – both, regarding governmental crisis management and the makers’ response. The latter followed the global pattern of community-based endeavours of designing and manufacturing PPE and other healthcare solutions as a collective response to Covid-19, typically making use of 3D printing technology, as shown above.
If the growth of academic literature on this response can be taken as an indicator, there has been a growth in this particular niche market in many regions and countries. The material on Brazil appears to be especially rich (Braida & Unanue, 2021; Ferreira dos Santos et al., 2020; Moura et al., 2020; Prado et al., 2020), with reports from Pernambucco (Ferreira et al., 2020), Porto Alegre (Freire et al., 2020), Belo Horizonte (Braga et al., 2020), Florianopolis (Pupo, 2020), or Rio de Janeiro (Braga et al., 2020; Cipolla, 2020; Santos et al., 2020). Herrera et al. (2021) adopt a broader view on Latin America. Rebola et al. (2020) and Doehler and Jones (2021) describe the situation in Cincinnati, while Budinoff et al. (2021) provide a perspective of the community-driven response in whole of the United States. Sari et al. (2021) report an example from Indonesia. Tsuda and Skauragi (2020) describe the response in Japan. Chalet et al. (2020, 2021) analyse and interprete the situation in France, and Richterich (2020) observed the hackers’/makers’ projects in the UK. The Open Source Medical Supplies project collected case studies from Germany, Brazil, India, Romania, France and Spain (‘National Maker Response Case Studies’, n.d.).
2.3 Peer-produced design – for disaster or for transition?
So, from a transition perspective, preconditions and generative mechanisms appeared to be in place: There was a window of opportunity. 3D printing had become a dominant design in various niches, and it had found hybrid and add-on use with existing manufacturing technologies. There was a growth in the niche markets of community-based, collective, and distributed 3D printing of personal protective equipment for healthcare and related sectors. So, could that novel configuration of PPE peer-production spur as radical innovation from its niches into the wider sociotechnical regime?
In their study, Moura et al. (2020) identify two cases of transition design in their collection of 113 design responses to the pandemic. So, they conclude that across their selection, designers “neglected the transition design approach in favor of design for disaster’s one” (p. 339).
Budinoff et al. (2021) reviewed 145 publicly available news stories on community-driven 3D printing of PPE, and surveyed 74 individuals involved in these efforts. They focus mainly on the technical aspects of 3D printing and improvements that could be made, like the control of process parameters and quality, optimization of designs, minimization of adjusting designs to specific printers and design documentation. They discuss the community-driven response as an add-on to existing manufacturing technologies, specifically from a perspective of maximizing production. However, they acknowledge that community-driven use of 3D printing in response to emergencies is promising, particularly because “nearly all surveyed individuals characterized their group’s effort as successful” (p. 35). So, from a manufacturing perspective, Budinoff et al. (2021) acknowledge the transitional potential of community-driven PPE production using 3D printing.
Chalet et al. (2020) described and analysed the process of self-organization among makers in France. They find that makers while driven by their individual initiative adopted organizational patterns they were familiar with – from industry, with a focus on productivity and efficiency, from the service economy, for example by establishing digital platforms to match supply and demand, or from clubs and associations, by working work on their immediate environment and using word of mouth. After the first wave of Covid-19, when demand for face shields fell, makers halted their activities or shifted from distributed manufacturing to humanitarian undertakings like sending face shields to Latin America or Africa. The main effect of the makers’ response in France, so Chalet et al. (2021), was that “makers acquired, with the same enthusiasm, the recognition of society and a greater awareness of themselves” (p 94). They demonstrated, that “makers have succeeded in being effective quickly by relying on the combination of self-organization and conviviality, which is a striking counterexample in the face of the dominant models of the organization of work in capitalist society, where hierarchy, hyper specialization and lack of meaning contribute to reducing work to smithereens” (Chalet et al., 2020, para. 27). So, from a sociological perspective, Chalet et al. recognise the strength of the transition narrative of the makers’ response.
Richterich (2020) closely followed civic DIY volunteers stepping in to counteract healthcare supply shortages in the UK and analysed that response through the lens of critical making (Ratto, 2011). Critical making was particularly expressed in the DIY volunteers’ careful deliberations, together with healthcare professionals, about which medical equipment could be practically and ethically produced in a hacker-/makerspace setting in order not to compromise the safety and efficacy of its use. The study also highlights the efficiency of open design for civic innovation and co-production, contradicting the medical manufacturers claim that patents are indispensable for innovation in the sector. Richterich (2020) argues, that DIY making of medical equipment was political, as it was “inextricably linked to austerity politics and the UK’s strained healthcare system” (p. 165). So, following Richterich, 3D printed face shields from a maker space are material signs of a destabilisation in the political regime that created a window of opportunity for niche-innovation.
In summary, several studies have shown that peer-production of personal protective equipment prima facies as a helpful response to disaster. However, this response revealed substantial technical potential, a new social narrative, and latent political power. So, in order to answer the questions whether PPE peer-production was a “transition”, spurring radical innovation from its niches into the wider sociotechnical regime, and if it was, in that sense, an “infrastructure project”, more data was needed. Such data would ideally be more maker focused and include more of makers’ own voices.
3 Method
Having been involved in the making scene and the research about it made me aware of the extra strain every new study or survey puts on the actors who are doing and organizing making. Still, aware of the drawbacks of working with already recorded evidence (see also the discussion section) I decided to first look for an extant body of makers’ voices. A rich source of more information on the civic response to Covid-19, and particularly those of makers, came into focus in the form of a series of online panel discussions organized for the Make: Community. The series had title “Plan C Live” where C stands for civic action (Dougherty, 2020). It had the theoretical advantage to come from the heart of what Hepp (2018) identified as the driver behind the pioneer community of makers. The panels were held on Zoom, streamed on Facebook, and subsequently published to YouTube. Between April and November 2020, Dale Dougherty – together with colleagues Mike Sense, editor at Make:, and Dorothy Jones-Davis, executive director of Nation of Makers – held 23 panels on the makers’ response to Covid-19 (full list of panels see Appendix: Plan C Live Panels).
The panels covered a variety of topics, about half of them (11) addressing the local response in particular cities, by specific organisations, and in selected European countries. Others were discussing specific projects like ventilators, masks, or even the rapid development of a vaccine (3). Several shows discussed issues specific to makerspaces (4), maker education (3), and community matters (2).
In a process following the lines of emergent qualitative document analysis (Altheide et al., 2008), I selected and analysed the 5 panels that addressed the makers’ response in European countries (the other panels were US-centric). I had several reasons to support this choice as one of theoretical sampling. First, my personal knowledge of the situation of makers in Europe is much more involved than that’s the case for the US. In the meantime, a detailed analysis of the production efforts for PPE in makerspaces in response to Covid-19 in the US has been published (Budinoff et al., 2021). Second, the (government) response to the pandemic in the United States appeared to be different to the response in many European countries – with less stringent lockdown measures than in Europe, and measures released more slowly than in continental Europe (see Footnote 3). Third, differences in the healthcare system between the US and Europe might have led to inverse stereotypical misinterpretations we tend to attribute to US-centric analyses of Europe. The 5 Europe-centric panels amounted to about six hours of video material (see Table 1).
Table 1. “Plan C Live” panels. The shows were hosted by Dale Dougherty (in the case of France, marked with *, by Mike Sense), and co-hosted by one (in the case of the UK: two [2]) local co-host(s); the co-hosts are included in the number of panellists.

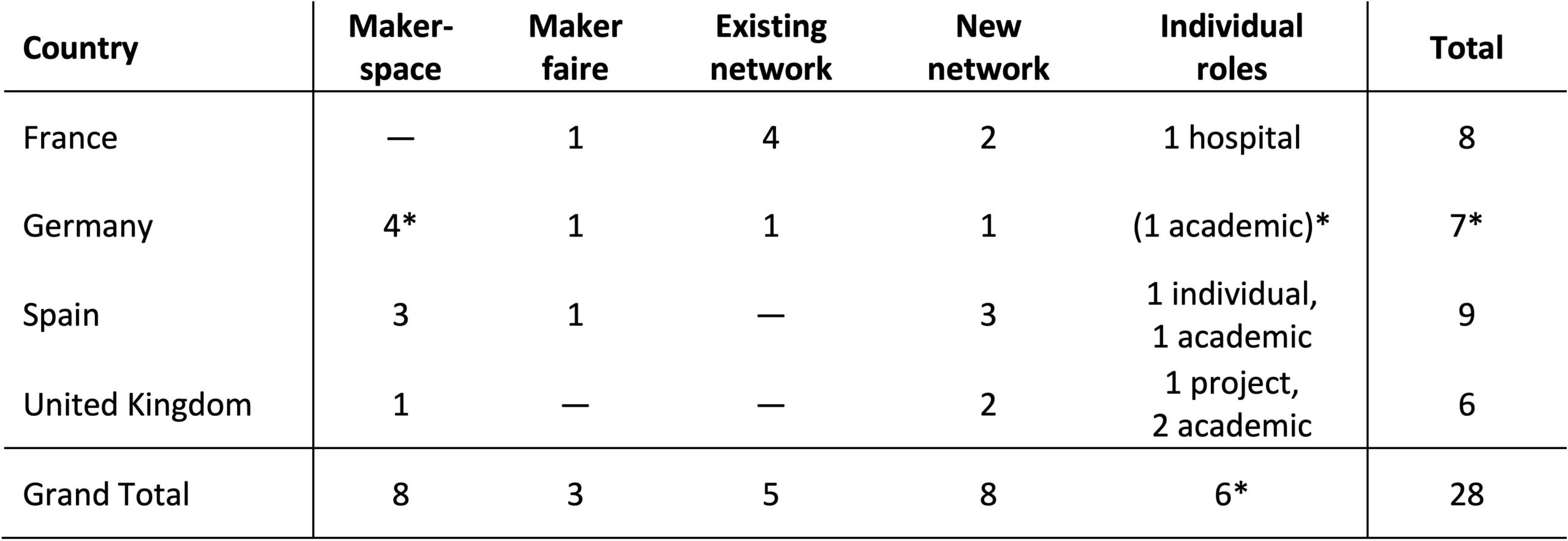
Per country, the “Plan C Live” panels brought together between six and nine representatives of the “maker movement” – typically people involved in maker spaces and maker faires or representatives of networks of makers, many of these networks had been newly established in response to Covid-19. Others were representatives from academia – with one individual representing an academic maker space – or hospitals, and finally two panellists were invited as a highly connected individual and initiator of one particular project, respectively (see Table 2).
The panels followed a common pattern. After the opening by the host, the local co-host would give an overview of the developments in the country. Thereafter, the individual panellists would have approximately ten minutes to present their own activities. Then, a discussion of the developments in the respective country followed. The panels would conclude with questions and answers from the host and from supposed outside participants.
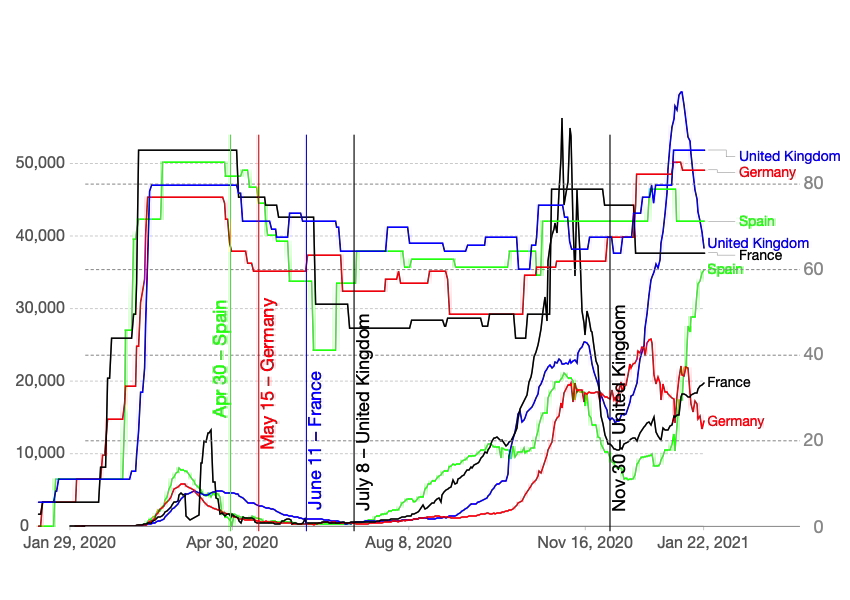
The four initial panels were held in the period from April to July of 2020. This was typically just after the first wave of registered Covid-19 cases and in each of the countries when the initial and rather drastic lockdown conditions were being eased. Those lockdown conditions included school and workplace closures, restrictions on public gatherings, transport restrictions, and stay-at-home requirements. According to the Oxford COVID-19 Government Response Tracker (Hale et al., 2021) which is calculated from nine specific measures, the lockdown measures reached levels of 87.96 and 85.19 in France and Spain, and 79.73 and 76.85 in the United Kingdom and Germany, respectively (see Figure 1).[3]
Table 2. Roles of “Plan C Live” panellists. In Germany, one makerspace was located at a university, which is marked with * in the table below. Its representative is only counted once in the respective totals as representative of a makerspace.
For this paper I created an extended description of each show based on an individual repeated viewing of the recording and a content analysis of the related auto-generated closed captions file provided by YouTube and downloaded via the downsubs.com service. An exception is the 30 November UK show that reviews the development since the first UK show in July; since no recording of that show has been posted to YouTube at the time of writing, repeated viewing and closed captions were not available. I analysed the data in several round of data analysis. First, I created an overall description of the panels based on annotating the videos and the closed caption files. In the second round, I split the closed caption files into “responses” (i.e., the individual projects the panellists talked about), i.e., shifting the unit of analysis from panel to response, and I content coded these responses. In a third round, I extracted representative, literal quotes from the captions.
4 Results
The “Plan C” panels were held in the immediate aftermath of lockdown periods of several weeks during which most of public life was halted – essentially confining residents to their homes, halting all non-essential business, closing schools, and banning gatherings of people altogether. It is in that extraordinary situation that the makers’ response emerged.
Digital communication infrastructures were essential for makers to establish contact. Telegram, Facebook, and WhatsApp were the platforms where makers gathered initially. However, makers quickly moved on to build their own digital platforms (see Table 3). Those platforms typically had more structured discussions facilities, organized into topics as in an Internet forum, they included or connected to repositories for blueprints of product designs, or they offered mapping facilities to coordinate makers’ activities or even product demand on geographical proximity, an essential feature when lockdown conditions forbade any long-range displacement. The situation in Germany was different, however. The federal government-organized a virtual hackathon “WirVsVirus” (20-22 March 2020) which became the place to gather, and makers kept using the digital infrastructure that had been set up for the hackathon (essentially a Slack environment) for their further communications.
Table 3. Type of makers’ response in terms of projects presented in the four early “Plan C Live” panels.

The large majority of makers were essentially making products – mainly face shields, as various studies confirmed (Budinoff et al., 2021; Galdon et al., 2020). A third of the responses in the panels concerned products only. Ten of the 17 product responses discussed in the “Plan C” panels were about face shields. Three covered other types of PPE (masks, garments), two were on respiratory apparatus (masks and ventilators), and two were other 3D printed products, e.g., hands-free door openers (see Table 3).
The largest proportion (just above 40 %) of the responses discussed in the panels consisted of services, half of them directed towards the logistics concerned with distributing PPE and the coordination of makers’ efforts. The remainder is almost evenly split between services to foster partnering with (manufacturing) SMEs and a large variety of other services – ranging from explicitly keeping 3D printers available for prototyping, industrialisation of products, and point-of-care manufacturing, to academic collaboration, and supplying PPE to third world countries (see Table 3).
Other responses presented in the panels included recording personal stories of people, dealing with social media, and more analytical approaches to the makers’ response from sociological and political perspectives.
4.1. Cooperation
The makers’ response was mainly triggered by the feeling and conviction of makers that “the world is in need of help, and this is a help we can provide” (SP9). A key ingredient to providing that help was obviously to bring people together. Not only the idea of producing help at scale through a large network of participants required cooperation. There was also a need of a variety of talents beyond the capability to successfully operate a 3D printer. Organising a factory-like flow of materials, procuring supplies, coordinating logistics, “all of these day-to-day skills that the people used in their normal economic life proved absolutely invaluable in putting this together” (UK3).
And cooperation required some amount of stewardship: “There were a lot of egos having a lot less sleep than they should have, talking to each other over the Internet, to people they never met before, and [it] just was kind of explosive sometimes. But I think we actually managed to get along quite well” (GE3).
Co-design as another form of cooperation was key to the makers’ response, involving doctors and other healthcare professionals when determining the needs and optimizing designs: “We have been every day to the hospital; in every night shift they tested the new version of the shields. Then we adapted them according to their needs and requirements. … So, we found a solution within about two weeks that were suitable to all the needs” (GE2).
Makers also realized that they were not capable to provide help alone, not even when operating in a network of individuals. Distribution of products was an issue. Some set up their own distribution network (FR5, FR6, UK4), while others got helped by the Red Cross (GE2) or the army (FR4). Scaling of production was another issue which different groups of makers approached differently. Some groups approached scaling by extending the network of volunteers, building “the decentralized Amazon of face shields” (UK4). Others involved local SMEs that could provide injection moulding to achieve larger production runs: “We somehow turned from producer of stuff to logistics operations” (GE6).
These observations echo what Chalet et al. (2020, 2021) remarked about organizing – new forms of mobilizing makers by using digital platforms, but also reverting to known patterns of organizing. Similarly, the use of technology to scale manufacturing – 3D printing versus injection moulding – shows new socio-technical configurations alongside traditional ones.
4.2. Resources
Support from local SMEs was also relevant regarding the supply of raw materials to produce face shields and other things: “Companies making filament donated filament. I think we caught like six or seven tons of filament that were distributed to different people” (ES2). Similarly, for producing face shields, a local bakery “donated a very large role of the plastic that we used for almost the entire project” (UK3), plastic the bakery normally was using for the transparent covers of their fancy cake boxes.
Such examples indicate, that largely, the makers’ response was funded through private donations, often in kind rather than in cash, through donations of filament, plastic foil, or services provided: “the mould for doing these [masks], only the mould, costs 5000 Euro, and the injection company, the president, paid” (SP5).
In France, one platform received a grant from a private research foundation which they redistributed to small projects that could apply for funding through the platform (FR7). Also, another project, concerned with point-of-care manufacturing, got privately funded (FR8). The German government created a 156 billion Euro Covid-19 fund; however, this fund was not accessible for NPOs (GE6), which is the formal structure of choice for most German makerspaces, unfortunately. Richterich (2020) reports the same for the UK.
Private donations were collected. But probably one of the most substantial resource was the time volunteers were willing and able to spend towards the various projects: “in two weeks we did the same work that we usually do in one year maybe” (SP6). However, this was not a stable workforce: “A great many of the talented people are on furlough” (UK6), so when businesses resumed operation, those people were much less available for volunteer work. This became clear in the second UK panel – people had less time at their hands when lockdown measures were relieved and other activities restarted, and donations from companies declined, a development similar to what Chalet et al. (Chalet et al., 2020) report for France.
Apparently, makers were able to capture a window of opportunity to make otherwise “idle” capacity of people and their 3D printers to participate in a new and very purposeful socio-technical manufacturing configuration. And they were able to stimulate manufacturing SMEs to participate in their efforts. However, the availability of these resources was more transitory than transitional.
4.3. Regulations
A topic touched upon several times in all the panels was regulations and standards in the medical sector. Particularly the scuba mask story ignited the ambitions at the time, not only of makers. Yet makers were also aware of the scientific scrutiny of the project (Germonpre et al., 2020), “that’s why we actually got in touch with the doctors … and we always wanted to confirm every prototype we were making” (SP8). Interacting with individual doctors and hospitals was the preferred strategy: “we were working with the hospital so closely, we did everything to hospital standards, and we were able to actually create a technical file that was of the quality that could be CE marked” (UK3). By CE marking, the manufacturer or importer affirms a products conformity with European health, safety, and environmental protection standards for products sold within Europe.
Many projects decided to use the Prusa face shield – probably not just because Prusa is a trusted brand in open-source hardware, but also because Prusa had received CE certification of their own production process, had certification that the shield conformed to European PPE standards, and even mentioned “two verifications with the Czech Ministry of Health” on their website (Prusa Research, 2020).
Attempts to interact directly with regulators were either held in private and could not be shared in the open as “there was some sensitivity” trying to convince regulators to join the communities (UK5), or they ended in confusion when the regulator was asked for advice for makers and responded with a standard answer “thank you for your mail, … remember to wash your hands” (FR4).
Makers were crucially aware of the strong regulations in the field of medical equipment and the reasons for these regulations. Working, and particularly co-designing with healthcare professionals was a necessary precaution to be able to provide safe and still quick solutions. However, meaningful interaction with regulatory bodies or even an attempt at reconfiguring the regulatory regime remained beyond reach for makers.
4.4. Achievements
A striking feature of all panels was an obsession of the panellists with numbers: how many visors they produced, how many tons of filament they used, how quickly injection moulding manufacturers could supply thousands of pieces. The most accentuated example of KPI-ing the makers’ response was: “8000+ volunteers 3D printed for the NHS & other healthcare workers 185,000+ face shields using 3000 km of filament enough to stretch from London to Rome and back again, or Edinburgh to Athens, Belfast to Moscow, or Cardiff to Ankara, combined printing time 60+ years in just 10 weeks” (UK4). Some panellists appeared impressed by the scale they could achieve if working together in large enough numbers – and by the scale of mass manufacturing processes – compared to the solo experience of 3D printing.
There was a notion across the “Plan C Live” panels that through working together on scale makers had made big steps and moved away from the image of “funny guys that make funny activity in Maker Faires” (FR3). Makers had shown their capability of redesigning objects quickly and effectively. Maker spaces were able to move from prototyping to production to a certain degree, although an increasing complexity of devices could render manufacturing capabilities the limiting factor. They have proven that they were developers and could act faster than companies and governments – “the maker movement reached some kind of maturity: it’s time to get the licence to drive” (FR6).
The makers’ response was – at least in one panellist’s view – a demonstration of “open R&D line” (GE3) – that could be relevant for a next wave of infections or any other crisis coming up. However, another panellist in a different panel contested that: “there has been never a moment in the last decade or ever … where the maker word has been so popular and so everywhere, I don’t know if most people could relate that maker were essential to the engineering and technological aspect or more the people wanting to help and take care of others. So, I’m not sure what you’re asking about these; would people say that this is like R&D? I’m not even sure about that” (SP4).
What were possible next steps for the makers’ response, as the market for face shields was saturated, the demand for PPE from hospitals and frontline workers from makers had declined as the “regular” supply chains recovered? Makers were looking for purpose in other fields of activity – moving on to other projects, like a bioreactor repurposing PET, 3D printed prosthetics for children, face mask kits for schools, Perspex separators for restaurants, and holders for Covid-19 test tubes. Others were considering “pivoting” to the global South, for example producing ventilators splitters, setting up a “mask house” at a refugee camp, or to developing projects for disaster relief. Action lines were sketched that both could fall under a “minimal ethical framework: we want to help people (and we don’t want it because we want to earn money)” (GE3) – first, to maintain the network of local initiatives as “makers for sustainability” as it proved to be resilient in a period of chaos attributed to a break-down of the capitalist system, and second to expand on humanitarian help as “makers for humanity” which would need more international coordination.
There is clearly a – sometimes cautious – recognition among makers that with their fast and numerous response to the PPE shortage in the early wave of the Covid-19 pandemic, they were able to achieve something they probably did not even dare to dream of: producing meaningful gear at some scale and in a collective endeavour that received positive press coverage across the board – e.g., 3500 articles in France alone between 17 March and 11 May 2020 (Chalet et al., 2020, n. 1).
5 Common threads
The European “Plan C Live” shows were held around the peak of the first wave of Covid-19 infections and related governmental “protection” measures – except for the last follow-up panel in the UK. The shows were created around the narrative that they would be streamed live and were announced accordingly on relevant social media channels. The shows were supposed to last one hour, so the co-hosts tried to cram all the achievements of their panellists into those sixty minutes – ending up both overrunning the hour (which for Zoom sessions and streaming on Facebook was not a particular problem) and cutting presentations and discussions short.
In all the four countries, the makers’ response started on a multitude of communication channels on various social media platforms, and often within only hours or at least a few days dedicated, centralized platforms were set up to unite makers nationally – not only in the four countries selected for “Plan C Live” shows, but all across Europe. This was certainly a reflection of the pattern how governments in Europe responded to the pandemic.
However, makers tended to organize nationally in Europe long before the pandemic; even the Maker Faire Rome that started in 2013 as the “European edition” in Rome felt more like the “Italian edition” since 2016.
Some of the makers responses built on large networks of individually operated 3D printers – either in a distributed network or at a more centralized mini-factory. Others, however, were intentionally employing industrial mass manufacturing to scale-up production, and intentionally reserving 3D-print capacity for development and prototyping. At least in one panel, the German one, there was an open disagreement between panellists which strategy would be the “better” or “more acceptable” one for makers as partnering with industry was felt as potentially betraying the “maker ethos” and depriving makers of a much-desired source of income.
A key feature of the makers’ response was their involvement with medical professionals – doctors and frontline workers. In many cases they started co-creation activities where makers would develop prototypes of equipment, have doctors or nurses test them and improve the equipment based on their feedback.
This was certainly no novelty for design and development of medical equipment, user-centric and co-design being well-established design strategies (Sanders & Stappers, 2008; Stappers et al., 2011). However, for some makers this might have been a new experience, as makers tend to operate “from their own itch” (Raymond, 1999), they “alleviate an everyday need, even if only from the idiosyncratic view of an individual” (Boeva & Troxler, 2021, p. 225). For many of the doctors and nurses, however, the experience of being asked to contribute, to co-design, would most probably have been a new experience as co-design activities often only happen at university hospitals. Moreover, Chalet et al. (2021) stress that the encounters between makers and medical professionals were also deeply emotional.
6 Preliminary interpretation
In the four early panels it was evident that makers were grasping the situation of supply shortages to make a meaningful contribution to society. As mentioned, they were eager – and able – to move away from the image of “funny guys that make funny activities in Maker Faires”, to overcome their privileged underdog position of white men spending their free time in manual leisure. In the height of the first lockdowns, the panellists were affirmative and hopeful that this shift had just begun.
In contrast, the list of “Plan C Live” panels tells a slightly different story – topics moving from makers helping the world back to more “internal” issues of re-opening maker spaces and educational activities. Equally, the second UK panel showed that the makers’ response – while meaningful and relevant in the first place – did not develop into a lasting new sector of the economy.
In the background section, I was wondering, if from a transition perspective, producing personal protective equipment for healthcare and related sectors was a novel configuration that could spur radical innovation from its niche into the wider sociotechnical regime, the maker movement “emerging as … an organic and organized and organizing power: What does this do to the economy, to the state, to the market, to the society as a whole?” (FR4).
From a theoretical point of view, the makers’ response appeared to have the ingredients of a window of opportunity, a dominant design, an add-on, and a developing niche market. In their very practical responses, makers indeed realised a new socio-technical configuration in organizing themselves, in putting social resources and technical means to good use. While respecting safe procedures and products in emergency circumstances, they did not attempt to reconfigure the regulatory regime. However, they established what Chalet et al. (2021) call “a digital archipelago of making” (p 94) that was “impressively demonstrating the potential of civic innovation” (Richterich, 2020, p. 166).
Inadvertently, makers stepped out of their shadow existence of consenting nerds.
They established – even if for just a short time – a novel socio-technical configuration that had no precedent, taking advantage of the window of opportunity that was presented by the pandemic. This very specific configuration, in its lasting effect was rather transitory than transitional. However, in exhibiting the power, efficiency, and effectiveness of that socio-technical configuration, the makers’ response demonstrated the emergent power of peer-production. It did not – in terms of my other question – establish an infrastructure akin to the Apache webserver; however, it left traces of infrastructure such as the OSMS database of open-source medical supplies.[4] Moreover, the makers’ response confirmed that making as peer-production was able to produce the seeds, the generative mechanisms for “inverse infrastructures” (Egyedi & Mehos, 2012) – the ability to mobilize personal capacities and technical capabilities and the co-ordination mechanisms to foster local response to a global challenge.
So, let’s recall Rip and Kemp’s technological regime (1998):
“A technological regime is the rule-set or grammar embedded in a complex of engineering practices, production process technologies, product characteristics, skills and procedures, ways of handling relevant artefacts and persons, ways of defining problems; all of them embedded in institutions and infrastructures” (p. 338).
In what way was the makers’ response evidently capable of creating – in transitional terms – an alternative technological regime?
The makers’ response was proposing a new “rule-set or grammar” of engineering practices, consisting of consumer grade 3D printing in combination with co-creation with frontline healthcare professionals, defining product characteristics according to the needs of those professionals, providing the necessary skills through makers while checking results in co-creation with the healthcare professionals. Makers were able to produce “relevant artefacts”, i.e, personal protective equipment for frontline workers. Makers managed to conciliate the demands of the extant institutions of healthcare and their own novel infrastructures of peer-production.
So, the real infrastructure and transition of the makers’ response to Covid-19 was not in the PPE and other contraptions they produced for frontline healthcare workers. And it was not in the massive, distributed, and connected putting-to-work of 3D printers. Makers themselves were even divided over the question if their efforts amounted to some sorts of R&D infrastructure. What makers proved in the early weeks and months of the pandemic is that they have the capability to respond locally to a global problem, that they have the capacity and capability for making and connecting, not only in a technical way, but also in a profoundly social way. This is, I believe, a novel infrastructure that might well be the foundation of a new socio-technical regime which is ready to supplant current regimes if conditions are right.
7. Discussion
When I say, “if conditions are right”, I am not referring to the pretty obvious regulatory questions. Regarding this issue, it was telling that, for example, when one panel was discussing regulations, the protection of manufacturers of PPE was mentioned prior to the protection of users (UK5).
Regarding “conditions are right”, I am rather referring to the political economic questions raised in the French panel (FR4). There was, in conventional economic theory terms, the opportunity for making big profits when demand was high, and supply was scarce (which for instance commercial parties exploited in the UK and the Netherlands). However, makers “gave the devices for nothing and spent much energy to work for nothing or for the glory. And this is very interesting from a sociological and economical point of view”. Makers, apparently, “did not want to monopolize, they want to be a community. So, the problem is that now, if they continue distributing everything for free, that they will kill themselves, and the problem is to build some kind of economic model; and in order to allow society to take benefit from all these skills and allowing them also to continue living a normal living” (FR4).
At the same time, another maker expressed their sentiment as being part of a hopefully transient regime: “From my perspective and many others, it was quite a weird situation where we wanted to be self-destructive in a very positive way” (UK4).
So, there is a political economic tension between understanding the makers’ response as just a transitionary emergency intervention in the sense of being positively self-destructive versus trying to build a new kind of economic regime. Indeed there was only one project in all the panels that explicitly was looking for commercialisation (UK6).
As all academic studies, this study has severe limitations, too. This study was relying on extant, potentially promotional material, which can be seen as an impediment. Would I not have asked more inquisitive questions? Certainly. But would respondents have replied more affirmative to my questions? Probably. I have chosen for analysing pre-recorded documents which are not liable to me influencing respondents, only to my own analytic bias.
The panels have been assembled by Make: and their community connections. It is known that Make: as a franchising organisation is at the base of medially constructing the “maker movement” (Hepp, 2016). So, there is a potential risk of panellists being part of a self-fulfilling prophecy of what the “makers’ response” to Covid-19 was supposed to be. Yet, knowing many of the panellists personally, I am convinced of their critical paricipaton in the panels.
So, in concluding, the makers’ response has brought tremendous help to frontline healthcare workers, quickly and at a moment when they most needed it. Face shields, door openers and ear savers were important parts of PPE that gave professionals the confidence of being able to continue to work safely.
However, the makers’ response so far was reactive, not proactive – even if it was anticipatory to the PPE shortages. It lacked strategic approaches, which has probably less to do with makers not being able to think, organise and act strategically, it’s more likely that their strategy counterparts in healthcare and regulation were not ready or in the mood of experimenting in times of the first peak of a pandemic. Strikingly, the way Covid-19 vaccines were developed, tested, and (emergency) approved might indicate otherwise. However, the parties involved in developing vaccines for sure were part of an incumbent socio-technical (and socio-economical) regime, reiterating their technocratic solutions.
Makers, to the contrary, strengthened the “movement” part to the notion of “maker movement”. Time will tell, if that concerns only the mediated part (as in the panels of “Plan C Live”) or if the parties who participated in the wider response – the makers, but also their networks, the SMEs, the healthcare institutions – will find ways to continue their cooperation beyond the pandemic. For the first time, makers stepped out of their shadow existence of consenting nerds and engaged in meaningful social and emotional peer-production. May that force be with them.
Endnotes
[1] It seems no coincidence that in the context of the pandemic politicians talk about a “new normal” that would replace how people used to live with their state-controlled, virus-compatible version.
[2] No recording available as of 31 July 2021.
[3] The US stringency index was at 72.69 from March 21 until June 14, 2020.
[4] https://opensourcemedicalsupplies.org/
References
Ali, A., Ballard, D. H., Althobaity, W., Christensen, A., Geritano, M., Ho, M., Liacouras, P., Matsumoto, J., Morris, J., Ryan, J., Shorti, R., Wake, N., Rybicki, F. J., Sheikh, A., & on behalf of the RSNA 3D Printing Special Interest Group. (2020). Clinical situations for which 3D printing is considered an appropriate representation or extension of data contained in a medical imaging examination: Adult cardiac conditions. 3D Printing in Medicine, 6(1), 24. https://doi.org/10.1186/s41205-020-00078-1
Altheide, D., Coyle, M., DeVriese, K., & Schneider, C. (2008). Emergent qualitative document analysis. In Handbook of emergent methods (pp. 127–151). The Guilford Press.
Anderson, C. (2012). Makers. Random House.
Ballard, D. H., Wake, N., Witowski, J., Rybicki, F. J., Sheikh, A., Ballard, D. H., Sheikh, A. M., Weadock, W. J., Ryan, J. R., Matsumoto, J. S., Souza, C., Wake, N., Levine, D., Ghodadra, A., Quigley, E. P., Christensen, A., Chepelev, L., Althobaithy, W., Jeyaraj, S., … RSNA Special Interest Group for 3D Printing Abdominal, H., and Gastrointestinal Conditions Voting Group. (2020).
Radiological Society of North America (RSNA) 3D Printing Special Interest Group (SIG) clinical situations for which 3D printing is considered an appropriate representation or extension of data contained in a medical imaging examination: Abdominal, hepatobiliary, and gastrointestinal conditions. 3D Printing in Medicine, 6(1), 13. https://doi.org/10.1186/s41205-020-00065-6
Bardzell, S., Nguyen, L., & Toupin, S. (Eds.). (2016). Feminism and (un)hacking. Journal of Peer Production, 8. http://peerproduction.net/issues/issue-8-feminism-and-unhacking/
Boeva, Y., & Troxler, P. (2021). Makers. In M. O’Neil, C. Pentzold, & S. Toupin (Eds.), The Handbook of peer production (pp. 225–237). John Wiley & Sons. https://doi.org/10.1002/9781119537151
Braga, M. F., Filho, E. R., Mendonça, R. M. L. O., Oliveira, L. G. R. de, & Pereira, H. G. G. (2020). Design for resilience: Mapping the needs of Brazilian communities to tackle COVID-19 challenges. Strategic Design Research Journal, 13(3), 374–386. https://doi.org/10.4013/sdrj.2020.133.07
Braida, F., & Unanue, M. G. (2021). Networks of digital manufacturing of face shields and the Covid-19: Design, maker culture and social mobilization. Strategic Design Research Journal, 14(1), 252–263. https://doi.org/10.4013/sdrj.2021.141.21
Braybrooke, K., & Smith, A. (Eds.). (2018). Makerspaces and Institutions. Journal of Peer Production, 12. http://peerproduction.net/issues/issue-12-makerspaces-and-institutions/
Budinoff, H. D., Bushra, J., & Shafae, M. (2021). Community-driven PPE production using additive manufacturing during the COVID-19 pandemic: Survey and lessons learned. Journal of Manufacturing Systems. https://doi.org/10.1016/j.jmsy.2021.07.010
Calvo-Haro, J. A., Pascau, J., Asencio-Pascual, J. M., Calvo-Manuel, F., Cancho-Gil, M. J., Del Cañizo López, J. F., Fanjul-Gómez, M., García-Leal, R., González-Casaurrán, G., González-Leyte, M., León-Luis, J. A., Mediavilla-Santos, L., Ochandiano-Caicoya, S., Pérez-Caballero, R., Ribed-Sánchez, A., Río-Gómez, J., Sánchez-Pérez, E., Serrano-Andreu, J., Tousidonis-Rial, M., … Perez-Mañanes, R. (2021). Point-of-care manufacturing: A single university hospital’s initial experience. 3D Printing in Medicine, 7(1), 11. https://doi.org/10.1186/s41205-021-00101-z
Chalet, L., Chareyron, V., Dutilleul, M., Fages, V., & Gayoso, É. (2020). « Make care »: Des visières contre le Covid-19. La Vie des idées. https://laviedesidees.fr/Make-care-des-visieres-contre-le-Covid-19.html
Chalet, L., Dutilleul, M., & Fages, V. (2021). Des visières à haut débit: Un regard sociologique sur la mobilisation des makers face à la crise sanitaire. Annales des Mines, Enjeux Numériques, 14, 89–94.
Chattopadhyay, S., Wood, L., & Cox, L. (Eds.). (2020). Interface: A journal for and about social movements. Organizing amidst Covid-19. Interface, 12(1). https://www.interfacejournal.net/interface-volume-12-issue-1/
Chepelev, L., Wake, N., Ryan, J., Althobaity, W., Gupta, A., Arribas, E., Santiago, L., Ballard, D. H., Wang, K. C., Weadock, W., Ionita, C. N., Mitsouras, D., Morris, J., Matsumoto, J., Christensen, A., Liacouras, P., Rybicki, F. J., Sheikh, A., Levitin, A., … RSNA Special Interest Group for 3D Printing. (2018). Radiological Society of North America (RSNA) 3D printing Special Interest Group (SIG): Guidelines for medical 3D printing and appropriateness for clinical scenarios. 3D Printing in Medicine, 4(1), 11. https://doi.org/10.1186/s41205-018-0030-y
Cipolla, C. (2020). Designing with communities of place: The experience of a DESIS Lab during COVID-19 and beyond. Strategic Design Research Journal, 13(3), 669–684. https://doi.org/10.4013/sdrj.2020.133.29
Corsini, L., Dammicco, V., & Moultrie, J. (2021). Frugal innovation in a crisis: The digital fabrication maker response to COVID‐19. R & D Management, 51(2), 195–210. https://doi.org/10.1111/radm.12446
CSSEGISandData. (2021). COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. https://github.com/CSSEGISandData/COVID-19 (Original work published 2020)
Doehler, S., & Jones, B. S. (2021). Production of protective face shields in Cincinnati, Ohio, USA from the 1819 Innovation Hub at the University of Cincinnati. In F. J. Rybicki (Ed.), Printing in Medicine and Its Role in the COVID-19 Pandemic: Personal Protective Equipment (PPE) and other Novel Medical and Non-Medical Devices (pp. 67–71). Cham: Springer International Publishing.
Dougherty, D. (2020, March 30). Plan C: Crisis mode for COVID-19. Make: DIY Projects and Ideas for Makers. https://makezine.com/2020/03/30/plan-c-crisis-mode-for-covid-19/
Egyedi, T., & Mehos, D. C. (2012). Inverse infrastructures: Disrupting networks from below. Eward Elgar. https://doi.org/10.4337/9781781952290
Ferreira dos Santos, A., Souza Ramos, I., Silva dos Santos, A. C., Faccin Borges, G., de Oliveira e Silva, I., & de Medeiros Guimarães, J. M. (2020, October 24). Equipamentos de Proteção Individual Impressos em 3D por Instituições de Ensino Federais para o Enfrentamento da COVID-19 | Ferreira dos Santos | Cadernos de Prospecção. http://web.archive.org/web/20201024042812/https://portalseer.ufba.br/index.php/nit/article/view/38373
Ferreira, T. C. B., Lima, K. M. P. de, & Araujo, K. M. (2020). Designers do Movimento Maker no Combate ao COVID-19: Análise de iniciativas em Pernambuco. Blucher Design Proceedings, 746–759. https://doi.org/10.5151/cid2020-58
Frazer, J. S., Shard, A., & Herdman, J. (2020). Involvement of the open-source community in combating the worldwide COVID-19 pandemic: A review. Journal of Medical Engineering & Technology, 44(4), 169–176. https://doi.org/10.1080/03091902.2020.1757772
Freire, K. de M., Franzato, C., & Remus, B. do N. (2020). Design amid Emergency. Strategic Design Research Journal, 13(3), 685–697. https://doi.org/10.4013/sdrj.2020.133.30
Galdon, F., Rodgers, P. A., & Bremner, C. (2020). A design history of the Covid 19 virus. Lancaster University. https://researchonline.rca.ac.uk/4520/1/adesignhistoryofthecovid19virus2020.pdf
Geels, F. W. (2002). Technological transitions as evolutionary reconfiguration processes: A multi-level perspective and a case-study. Research Policy, 31(8), 1257–1274. https://doi.org/10.1016/S0048-7333(02)00062-8
Geels, F. W., & Schot, J. (2007). Typology of sociotechnical transition pathways. Research Policy, 36(3), 399–417. https://doi.org/10.1016/j.respol.2007.01.003
Germonpre, P., Van Rompaey, D., & Balestra, C. (2020). Evaluation of protection level, respiratory safety, and practical aspects of commercially available snorkel masks as personal protection devices against aerosolized contaminants and SARS-CoV2. International Journal of Environmental Research and Public Health, 17(12), 4347.
Gershenfeld, N. (2005). Fab. The coming revolution on your desktop. Basic Books.
Gunbay, S., Hopkins, M., Hu, G., Gately, N. M., Devine, D. M., & Hayes, C. (2019). Additive Manufacturing of Tooling for Use in Mass Production Processes. In D. M. Devine (Ed.), Polymer-Based Additive Manufacturing: Biomedical Applications (pp. 73–96). Springer International Publishing. https://doi.org/10.1007/978-3-030-24532-0_4
Hale, T., Angrist, N., Goldszmidt, R., Kira, B., Petherick, A., Phillips, T., Webster, S., Cameron-Blake, E., Hallas, L., Majumdar, S., & Tatlow, H. (2021). A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nature Human Behaviour, 5(4), 529–538. https://doi.org/10.1038/s41562-021-01079-8
Hartig, S., Duda, S., & Hildebrandt, L. (2020). Urgent need hybrid production—What COVID-19 can teach us about dislocated production through 3d-printing and the maker scene. 3D Printing in Medicine, 6(1), 37. https://doi.org/10.1186/s41205-020-00090-5
Hepp, A. (2016). Pioneer communities: Collective actors in deep mediatisation. Media, Culture & Society, 38(6), 918–933. https://doi.org/10.1177/0163443716664484
Hepp, A. (2018). What Makes a Maker? – Curating a pioneer community through franchising. Nordisk Tidsskrift for Informationsvidenskab Ok Kulturformidling, 7(2), 3–18. https://doi.org/10.7146/ntik.v7i2.111283
Herrera, P. C., Dreifuss-Serrano, C., & Juarez, B. (2021). Design during COVID-19: Agents and allies in the role of designer, digital fabrication and distributed production. Strategic Design Research Journal, 14(1), 236–251. https://doi.org/10.4013/sdrj.2021.141.20
Kuhn, T. S. (Thomas S., 1922-1996. (1962). The structure of scientific revolutions. University of Chicago Press.
Kunovjanek, M., & Wankmüller, C. (2020). An analysis of the global additive manufacturing response to the COVID-19 pandemic. Journal of Manufacturing Technology Management, 32(9), 75–100. https://doi.org/10.1108/JMTM-07-2020-0263
Moura, M., Perez, I. U., Melara, L. F., & Júnior, J. C. M. (2020). Contemporary Design in Quarantine: A Critical Review of Design Responses to Covid-19 Crisis. Strategic Design Research Journal, 13(3), 327–341. https://doi.org/10.4013/sdrj.2020.133.03
National Maker Response Case Studies. (n.d.). Open Source Medical Supplies. Retrieved 2 August 2021, from https://opensourcemedicalsupplies.org/national-maker-response-case-studies/
Perez-Mañanes, R., José, S. G. S., Desco-Menéndez, M., Sánchez-Arcilla, I., González-Fernández, E., Vaquero-Martín, J., González-Garzón, J. P., Mediavilla-Santos, L., Trapero-Moreno, D., & Calvo-Haro, J. A. (2021). Application of 3D printing and distributed manufacturing during the first-wave of COVID-19 pandemic. Our experience at a third-level university hospital. 3D Printing in Medicine, 7(1), 7. https://doi.org/10.1186/s41205-021-00097-6
Prado, G. C., Leme, F. D. P., Messias, L. Z., Miranda, N. S. da C., & Gonçalves, R. de B. (2020). Strategies of design for social innovation and design activism in the promotion of positive social capital during the COVID-19 pandemic in Brazil. Strategic Design Research Journal, 13(3), 364–373. https://doi.org/10.4013/sdrj.2020.133.06
Prusa Research. (2020, March 18). Prusa Face Shield. https://www.prusaprinters.org/prints/25857-prusa-face-shield
Pupo, R. T. G. (2020). The importance of collaborative design process and fabrication during COVID-19 emergency – case in Brazil. SIGraDi 2020 [Proceedings of the 24th Conference of the Iberoamerican Society of Digital Graphics – ISSN: 2318-6968] Online Conference 18 – 20 November 2020, Pp. 357-362. http://papers.cumincad.org/cgi-bin/works/2015%20+dave=2:/Show?sigradi2020_357
Ratto, M. (2011). Critical Making: Conceptual and Material Studies in Technology and Social Life. The Information Society, 27(4), 252–260. https://doi.org/10.1080/01972243.2011.583819
Rebola, C. B., Norton, R., Doehler, S., & Kubley, A. (2020). Tri-Design: Coordination between Healthcare, Design, and Regulatory Communities. Strategic Design Research Journal, 13(3), 474–487. https://doi.org/10.4013/sdrj.2020.133.14
Richterich, A. (2020). When open source design is vital: Critical making of DIY healthcare equipment during the COVID-19 pandemic. Health Sociology Review, 29(2), 158–167. https://doi.org/10.1080/14461242.2020.1784772
Rip, A., & Kemp, R. (1998). Technological change. Human Choice and Climate Change: Vol. II, Resources and Technology, 327–399.
Ritchie, H., Ortiz-Ospina, E., Beltekian, D., Mathieu, E., Hasell, J., Macdonald, B., Giattino, C., Appel, C., Rodés-Guirao, L., & Roser, M. (2020). Coronavirus Pandemic (COVID-19). Our World in Data. https://ourworldindata.org/coronavirus
Rodgers, P. A., Galdon, F., & Bremner, C. (2020). Design Research-in-the-Moment: Eliciting Evolutive Traces during the Covid-19 Crisis. Strategic Design Research Journal, 13(3), 312–326. https://doi.org/10.4013/sdrj.2020.133.02
Rossi, E., Nicolantonio, M. D., Ceschin, F., Mincolelli, G., Santos, A. dos, Kohtala, C., Jacques, E., Cipolla, C., & Manzini, E. (2020). Design Contributions for the COVID-19 Global Emergency (Part 1): Empirical Approaches and First Solutions. Strategic Design Research Journal, 13(3), 294–311. https://doi.org/10.4013/sdrj.2020.133.01
Rossi, E., Nicolantonio, M. D., Ceschin, F., Mincolelli, G., Santos, A. dos, Kohtala, C., Jacques, E., Cipolla, C., & Manzini, E. (2021). Design Contributions for the COVID-19 Global Emergency (Part 2): Methodological Reflections and Future Visions. Strategic Design Research Journal, 14(1), 1–18. https://doi.org/10.4013/sdrj.2021.141.01
Rybicki, F. J. (2021). 3D Printing in Medicine and Its Role in the COVID-19 Pandemic: Personal Protective Equipment (PPE) and Other Novel Medical and Non-Medical Devices. Springer Nature.
Sáez, C. G., & Cuartielles, D. (2020). Makers against Covid-19: Face shields as the international solidarity KPI. Strategic Design Research Journal, 13(3), 525–537. https://doi.org/10.4013/sdrj.2020.133.18
Sanders, E. B.-N., & Stappers, P. J. (2008). Co-creation and the new landscapes of design. CoDesign, 4(1), 5–18. https://doi.org/10.1080/15710880701875068
Santos, J. R. L. dos, Melo, J. V. C. de, Frajhof, L., & Kauffmann, A. R. (2020). Confronting COVID-19—The case of PPE and Medical Devices production using Digital Fabrication at PUC-Rio. Strategic Design Research Journal, 13(3), 488–501. https://doi.org/10.4013/sdrj.2020.133.15
Sari, M. W., Herianto, Dharma, I. B., & Tontowi, A. E. (2021). Applying an integrated production system based on social manufacturing to develop a medical device. Journal of Physics: Conference Series, 1823(1), 012117. https://doi.org/10.1088/1742-6596/1823/1/012117
sculpteo. (2021). The State of 3D Printing 2021 (p. 16). https://info.sculpteo.com/hubfs/downloads/The%20State%20of%203D%20Printing%202021.pdf?_ga=2.164485565.349060181.1627388705-275090730.1627388705
Sher, D. (2020a, March 14). [Updating] Italian hospital saves Covid-19 patients lives by 3D printing valves for reanimation devices. 3D Printing Media Network – The Pulse of the AM Industry. https://www.3dprintingmedia.network/covid-19-3d-printed-valve-for-reanimation-device/
Sher, D. (2020b, March 21). Isinnova shares 3D printed adapter to turn snorkeling mask into a non-invasive ventilator. 3D Printing Media Network – The Pulse of the AM Industry. https://www.3dprintingmedia.network/isinnova-shares-3d-printed-adapter-to-turn-snorkeling-mask-into-a-non-invasive-ventilator/
Stappers, P. J., Visser, F. S., & Kistemaker, S. (2011). Creation & co: User participation in design. Open Design Now: Why Design Cannot Remain Exclusive (pp. 140–148). BIS.
Sugrue M, O’Keeffe D, Sugrue R, MacLean L, & Varzgalis M. (2020). A cloth mask for under-resourced healthcare settings in the COVID19 pandemic. Irish Journal of Medical Science, 189(4), 1155–1157. https://doi.org/10.1007/s11845-020-02241-3
Thiel, J., Ravi, S., & Bryant, N. (2017). Advancements in Materials for Three-Dimensional Printing of Molds and Cores. International Journal of Metalcasting, 11(1), 3–13. https://doi.org/10.1007/s40962-016-0082-y
Throckmorton, A. L., Bass, E. J., Ferrick, B., Ramakrishnan, A., Eichmann, S., Catucci, N., Eshelman, B., McNamara, J., Sundquist, E., Beatson, N., Hirschhorn, M., Menon, P., Datner, E., Stevens, R., & Marcolongo, M. (2021). A Cross University-Led COVID-19 Rapid-Response Effort: Design, Build, and Distribute Drexel AJFlex Face Shields. Annals of Biomedical Engineering, 49(3), 950–958. https://doi.org/10.1007/s10439-021-02743-w
Tino, R., Moore, R., Antoline, S., Ravi, P., Wake, N., Ionita, C. N., Morris, J. M., Decker, S. J., Sheikh, A., Rybicki, F. J., & Chepelev, L. L. (2020). COVID-19 and the role of 3D printing in medicine. 3D Printing in Medicine, 6(1), 11. https://doi.org/10.1186/s41205-020-00064-7
Troxler, P. (2010, October 7). Commons-Based Peer-Production of Physical Goods: Is There Room for a Hybrid Innovation Ecology? 3rd free culture research conference, Berlin. http://papers.ssrn.com/abstract=1692617
Troxler, P. (2011). Libraries of the Peer Production Era. In (Eds.) B. van Abel, R. Klaassen, L. Evers, & P. Troxler, Open Design Now. Why Design Cannot Remain Exclusive (pp. 86–95). BIS.
Troxler, P. (2013). Making the Third Industrial Revolution the Struggle for Polycentric Structures and a New Peer-Production Commons in the Fablab Community. In J. Walter-Hermann & C. Büching (Eds.), FabLab. Of Machines, Makers and Inventors (pp. 181–194). Bielefeld: transcript Publishers. https://www.transcript-verlag.de/chunk_detail_seite.php?doi=10.14361%2Ftranscript.9783839423820.181
Troxler, P. (2015). Beyond Consenting Nerds: Design Patterns for New Manufacturing. Inaugural Lecture. Rotterdam University Press. http://www.petertroxler.net/wp-content/uploads/2015/11/Internetversie-Peter-Troxler.pdf
Troxler, P. (2016a). Offene freie Technik. In A. Baier, T. Hansing, C. Müller, & K. Werner (Eds.), Die Welt reparieren. Open Source und Selbermachen als postkapitalistische Praxis (pp. 85–92). Transcript. http://www.transcript-verlag.de/978-3-8376-1/die-welt-reparieren
Troxler, P. (2016b, March 4). The workings of the making class. DIY antropocene, Nordic Summer University winter workshop, Gothenburg.
Troxler, P. (2017). Making as Social Fabrication: Towards a new Fab Commons? In (Eds.) A. Briceño & T. Vivanco, Fabricating Society (pp. 78–88). Fundacion DID. http://www.fundaciondid.cl/wp-content/uploads/2017/07/FabricatingSocietyResearchBook.pdf
Troxler, P. (2019). Building Open Design as a Commons. In L. Bogers & L. Chiappini, The Critical Makers Reader: (Un)Learning Technology (pp. 218–226). Institute of Network Cultures. https://networkcultures.org/blog/publication/the-critical-makers-reader-unlearning-technology/
Troxler, P. (2018). Fab Lab Research Papers. From Experiment to Expression. Proceedings from the Fab14 + Fabricating Resilience Research Papers Stream, 4–12. https://doi.org/10.5281/zenodo.1344101
Troxler, P., & Maxigas (Eds.). (2014). Shared Machine Shops. Journal of Peer Production, 5. http://peerproduction.net/issues/issue-5-shared-machine-shops/
Tsuda, K., & Sakuragi, M. (2020). Co-Design of Do-It-Yourself Face Shield in Japan Under COVID-19 Pandemic. Strategic Design Research Journal, 13(3), 502–510. https://doi.org/10.4013/sdrj.2020.133.16
Appendix: Plan C Live Panels
Table 4. “Plan C Live” panels. The shows marked with * were hosted by Mike Sense, those marked with ** were hosted by Dorothy Jones-Davis. The EU-centric shows, marked in bold, were co-hosted by one (in the case of the UK: two) local co-host(s); the co-hosts are included in the number of panellists. The topic codes are C for community matters, E for maker education, L for local response (cities, organizations, EU countries), M for maker spaces, and P for specific projects.
